Health Definitions
- Infant Mortality Rate: the Death rate of infants below the age of 1 per 1000 live births a year
- (Highest in sub-Saharan Africa with 102%)
- Life Expectancy: Average number of years a person is expected to live for
- (Highest in Japan at 83 years; Lowest ones include Chad at 50)
- Disability Adjusted Life Years: A health measure based on healthy life lost due to illnesses
- (Higher in areas with pollution e.g. Beijing)
- Calorie Intake: Food intake (in calories) per person a day
- (USA 3500~ calorie; Afghanistan 1500~ calories)
- Access to safe water: Percentage of the population with access to water that is affordable, adequate and disease-free
- (100% in MEDCs like Norway; only around 50% at sub-Saharan Africa)
- Access to health services: Ratio of doctors to patients in the population
- (China 600 : 1; Mozambique 50000 : 1)
- Health Adjusted Life Expectancy: An indicator that combines multiple statistics to calculate life expectancies for specific groups of a population in a country. (age, sex, socio eco)
- (E.g. Higher in middle ages, longer in richer countries, those with access to education and health)

Variations in Health
Life expectancy stats:
- Lowest in sub-Saharan African
- China and Asia, in general, was really low in 1950
- Japan, Australia, and Canada have really high life expectancy today
- In the last 60 years, Asia has a much higher life expectancy

Life expectancy has increased at both national and global scales, although they might be different at the local level. This is due to rising incomes and better lifestyles achieved with such incomes. Reasons for life expectancy rises to include:
- Clean water
- Access to sanitation
- Healthcare
- Better living conditions
Explaining Life Expectancy: Income

As shown in the graph above, people with low income have a lower life expectancy. People struggle to purchase basic necessities such as clean water or good quality food. As income increases, lifestyle choices about those purchases begin to be more important than the level of income itself. This means that despite an increasing income, a poor choice may lead to a drop in life expectancy due to lifestyle factors.
- Spending more on healthcare, including infrastructure and training
- Aid programs are given
- Most basic healthcare provided for free by governments
- Access to sanitation and water
- Better incomes correlate with better jobs
Explaining Life Expectancy: Lifestyle

- Activities (smoking, exercise)
- Diet (access to food might be double-edged)
- Healthcare provision
Prevention vs Cure

Prevention because…
- Takes less effort than curing diseases (Isolation/surgeries)
- Cost-effective in advertisements/awareness programs (MMR)
- Higher chance of surviving if diseases not contracted / No guarantee of survival
Curing because…
- No money needed for prevention
- No obligation on government (unethical though)
- Hard to educate poorer people about prevention (Africa)
- Fast-paced diseases which require prior knowledge can’t be prevented (Ebola)
- Remote areas make it hard to spread awareness
- Unexpected diseases due to geographical factors/ it being new (HIV)
Global availability of food

Global patterns of calorie intake
- Nauru and other Pacific Island Nations is the fattest country (61%), Sub Saharan Africa too thin, Japan lowest in OECD
Definitions:
- Malnutrition: Not enough intake of one type of food (can also include overconsumption)
- Temporary Hunger: Short-term decline in food availability in an area, leading to hunger
- Chronic Hunger: Undernourishment due to not ingesting enough food, leading to hunger
- Famine: Long-term decline in food availability in a region, leading to tons of malnutrition
Food security: When all people have safe, sufficient access to nutritious food to meet dietary needs and food preferences for a healthy life.
Areas of food sufficiency and deficiency

Tools used to increase food output
- HYV crops
- Fertilizers, Pesticides, Herbicides
- Irrigation
- Technology
Green revolution

The Green Revolution, or Third Agricultural Revolution, is a set of research technology transfer initiatives occurring between 1950 and the late 1960s, that increased agricultural production worldwide, particularly in the developing world, beginning most markedly in the late 1960s.
After World War II, newly implemented technologies, including pesticides and fertilizers as well as new breeds of high yield crops, greatly increased global food production.
IR8 Rice Case study:
IR8 is a high-yielding semi-dwarf rice variety developed by the International Rice Research Institute (IRRI) in Mexico in the early 1960s. In November 1966, “the variety was first introduced in the Philippines and India.” Promoters such as the IRRI and farmer benefactors of IR8 have called it miracle rice, and celebrate it for fighting famine.

Locations of IRRI research stations in the Yaqui Valley and Chapingo.

- India used Mexican Rice IR8, yields 2x more grain
- 55% adoption in India, only 13% adoption in Thailand due to it not being suitable for monsoon.
- IR8 required the use of fertilizers and pesticides
- Annual rice production in the Philippines increased from 3.7 to 7.7 million tons in 20 years.
- The switch to IR8 rice made the Philippines a rice exporter for the first time in the 20th century.
Main Advantages
- Higher yield
- Quality of life increase due to income increase
- Less hunger as more foreign currency leads to better infrastructure (GDP +)
Main Problems
- Can’t afford it as it requires a lot of water and stuff
- Fertility declines due to overuse of soil
- Poorer countries dependent on richer countries for input
- Machinery leads to unemployment
Why are there food deficiencies?

Multiple environmental, political, social, and economic factors such as:
Social factors
- Less-educated about farming techniques and HYV farming (India)
- Reliance on aid by other countries leads to donation fatigue
- Increased wealth leads to more expensive food consumed, less for everyone back then
Political factors
- Use of biofuel by the USA instead of food
- Underinvestment in agriculture (3% in 2006)
- Less efficiency due to division of land (Zimbabwe 1990s – more farmers per plot of land after division 6000 vs 245000)
- War prevents resources coming in, the land being bombed, farmers not working
Economic factors
- Increasing food prices by inflation
- Speculative trading in agricultural commodities (most poor farmers uneducated)
- Diversification of the economy towards secondary and tertiary sectors
Environmental factors
- Natural hazards
- Climate change (affects LICs more)
- Soil degradation due to HPV/ Overfarming
- Introduction of pest species may cause additional problems (New Zealand in the 1980s)
Demographic factors
- Rising demand for food due to population increase
- Migration (old dependents left)
Famine case study (the Horn of Africa, 2011)

The famine of Africa in 2011 caused more than 100,000 deaths and approximately 9 million affected in some way. As there was a food crisis alongside a civil war, it caused forced migration and overcrowding at refugee camps, leading to more diseases. It was one of the worst famines in 60 years.
Drought

- Lack of rainfall leading to driest year.
- Lack of food production, 60% arid
Conflict
Tens of thousands of people are believed to have died in southern Somalia before famine was declared. This was mainly a result of Western governments preventing aid from reaching affected areas in an attempt to weaken the Al-Shabaab militant group, against whom they were engaged.
- Without a functioning government
- Denied access to areas under Al-Shabaab (al-Qaeda affiliated), no aid arriving
- Mass migration and social problems caused by it
Demographics
- The population in this region has doubled since 1970
- Livestock farmers cannot find areas for livestock hence they migrated.
Poverty and global markets
- No access to tech or resources (irrigation, machines)
- Lack of Food aid and cheaper production in MEDCs
- Usually grown for export due to foreign companies (China)
Production and markets
.jpg)
There are many factors affecting the production and availability of food. These include:
Subsidies

Trading blocs (free trade among members) such as the EU made a Common Agricultural Policy that guaranteed prices and thence a guaranteed market. There were export subsidies to make prices competitive. Other examples include ASEAN, NAFTA. (Common fisheries policy is another example)
Results:
- Overproduction of food, unsustainable
Trade Barriers (taxes on imports, restrictions)

Protects home industries and increases self-sufficiency, employment opportunities.
Results
Reduction in production as quota restricts exports of a country, specialization will cause problems if prices drop or tax increases.
Bilateral and Multilateral arrangements

Bilateral agreements from one producer and consumers (Sainsbury and bananas from St Lucia) increase production. Multilateral agreements are when consumers agree to import goods from countries. ACP- (African, Caribbean, Pacific) produced bananas favored in EU over US TNCs.
Addressing Imbalances
To alleviate food shortages, food aid, free and fair trade are of key importance.
Food aid

World Food Programme has emergency feeding programs (2008- 755 million), victims of Sudan, etc. However only to most desperate people.
Free Trade

Trade liberalization, lowering farm subsidies in the USA and undoing some of the protectionism of the EU's CAP should help poor farmers in the future, but the direct impact could be to raise food prices in the developing world, as producers focus on western markets.
Fair Trade

Fair or ethical trade can be declined as a trade that attempts to be socially, economically, and environmentally responsible. It is trading in which companies take responsibility for the wider impact of their business. Ethical trading is an attempt to address the failings of the global trading system.
Sustainable Agriculture

Definitions:
Energy efficiency ratios: Measure of outputs vs inputs
Sustainable yield: Amount of yield that can be taken from the land without reducing the ability of the land to produce the same amount of goods in the future without inputs.
Food miles: The distance that food travels from where it’s produced to where it’s consumed. Dependent on oil usually so unsustainable. Eg, Christmas dinners are unsustainable.
Global Patterns of Disease (Affluence and Poverty)
The most common diseases are heart disease that affects MICs mostly, LICs suffer from a wider range of diseases.
Definitions:
Communicable disease: Disease that is transmittable (blood, bodily fluid)
Non-communicable disease: Diseases that are not transferable (autism)
Prevalence: Number of cases per 10000 people
Incidence: Total number of cases a year
Pandemic disease: Viral diseases worldwide
Endemic disease: Native diseases that stay [Using the epidemiologic transition, there is a correlation between development and mortality rate.]
Diseases of affluence
Diseases of affluence are associated with non-communicable diseases as the prevalence of communicable diseases is lower in richer societies.
Usually elderly get it (good medical care). E.g. Heart disease and cancer. Due to unhealthy lifestyles, these diseases occur:
- smoking, leading to cancer
- overeating, leading to obesity-related diseases
- drinking excess alcohol, leading to liver problems
Diabetes

Diabetes is a good example. Firstly, most people are unaware that Type 1 is not related to lifestyle factors, while Type 2 has risk factors such as a poor diet and lack of exercise. Secondly, even Type 2 can develop in individuals who have healthy lifestyles.
Diseases of poverty

Diseases of poverty are caused when no protection is given to conditions, often linked to poverty conditions. E.g. poor housing, water supply, food, education
Usually, people in LICs get it.
The Spread of Disease
Definitions:
Diffusion: By Relocation: Diseases move to a new area, leaving original behind (humans migrate)
Expansion: Move to new areas while remaining in the original area (HIV)
Barriers: Factor that causes the prevention of a disease
Epidemic: Increase in the number of cases of disease over what is expected
Barriers to Disease
/cdn.vox-cdn.com/uploads/chorus_image/image/66548221/1208078022.jpg.0.jpg)
- Quarantine
- Lack of legal entry
- School Closure
- Protection devices (face mask, sanitizer)
- Public awareness campaigns
- Injections and medication
- Transport and environment
Case Study: Malaria
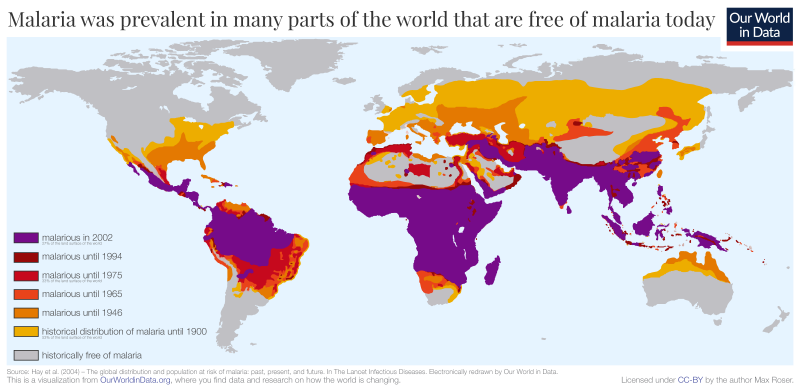
Malaria Kills 3 million annually mostly in sub-Saharan Africa. It is widespread in tropical countries, costing 1.1 billion annually. This is worsened through the factors described below.
Factors causing:
- People not immunized to malaria
- Virus becoming more drug-resistant
- Mosquitoes spreading into other areas
- Agricultural schemes
- International travel and trade increases
- Not safe sanitation
Impacts:
- Death of many including children which could have been cured (20% kids Africa deaths/yr)
- Medical costs, lost productivity and opportunity cost
Limiting the spread of malaria:
- DDT Chemical (Found to be carcinogenic)
- Nets
- Management of water areas
- Introduction of predator species
- Faster treatment through improved access
- Rollback malaria initiative
- Kenya Malaria Initiative (NATIONAL SCALE)
The Kenya Malaria Strategy

The Kenya Malaria Strategy (2014-2018) involves several interventions:
Vector Control

- 80% get ITNs (Insecticide Treated Nets)
- Universal ITN coverage for groups in malaria-endemic and epidemic-prone counties through regular ITN distribution campaigns, carried routinely through antenatal care clinics, social marketing of nets particularly in designated rural counties, and commercial sales of ITNs in the private sector.
Case Management

- ensure that all suspected malaria cases receive a diagnosis and effective treatment
- community health volunteers receive training and supervision for case management of malaria, prevention, behaviour change communication, record keeping and reporting
Advocacy, Communication and Social Mobilization
- emphasis will be placed on using interpersonal communication approaches by volunteers, community-based organizations and special interest groups to target hard-to-reach populations
- traditional channels of communication will be used
- Surveillance to track malaria activities
Millennium Villages Project in Sauri, western Kenya

The management strategies applied in Kenya can be seen through the example of Millennium Development Villages (reduces epidemics one village at a time)
The village is warm and humid hence more malaria occurs. It covers 11 villages. Through the changes made to not just malaria intervention, but also poverty reduction efforts, malaria in Sauri reduced from 50% to 8% between 2000 and 2012.
This is helped by rapid diagnostic tests (RDT) allowing 100 cases instead of 40 cases per day to be looked at.
Case Study: AIDS and HIV
AIDS/HIV has impacted many people around the world, more in some areas than others. Over 70% of HIV cases are in Africa, a very skewed amount compared to others. This causes multiple impacts on people.
Botswana
Causes:
- The exchange of body fluids (unprotected sex), multiple partners, prostitution (status of women)
- From mother to child during pregnancy (also through breast milk)
- Through contaminated needle use (especially by drug users) and blood transfusions
- In the case of Botswana the first and second causes are the most important.
- Lack of preventative care, advice (condoms) or medication (education)
Impacts: 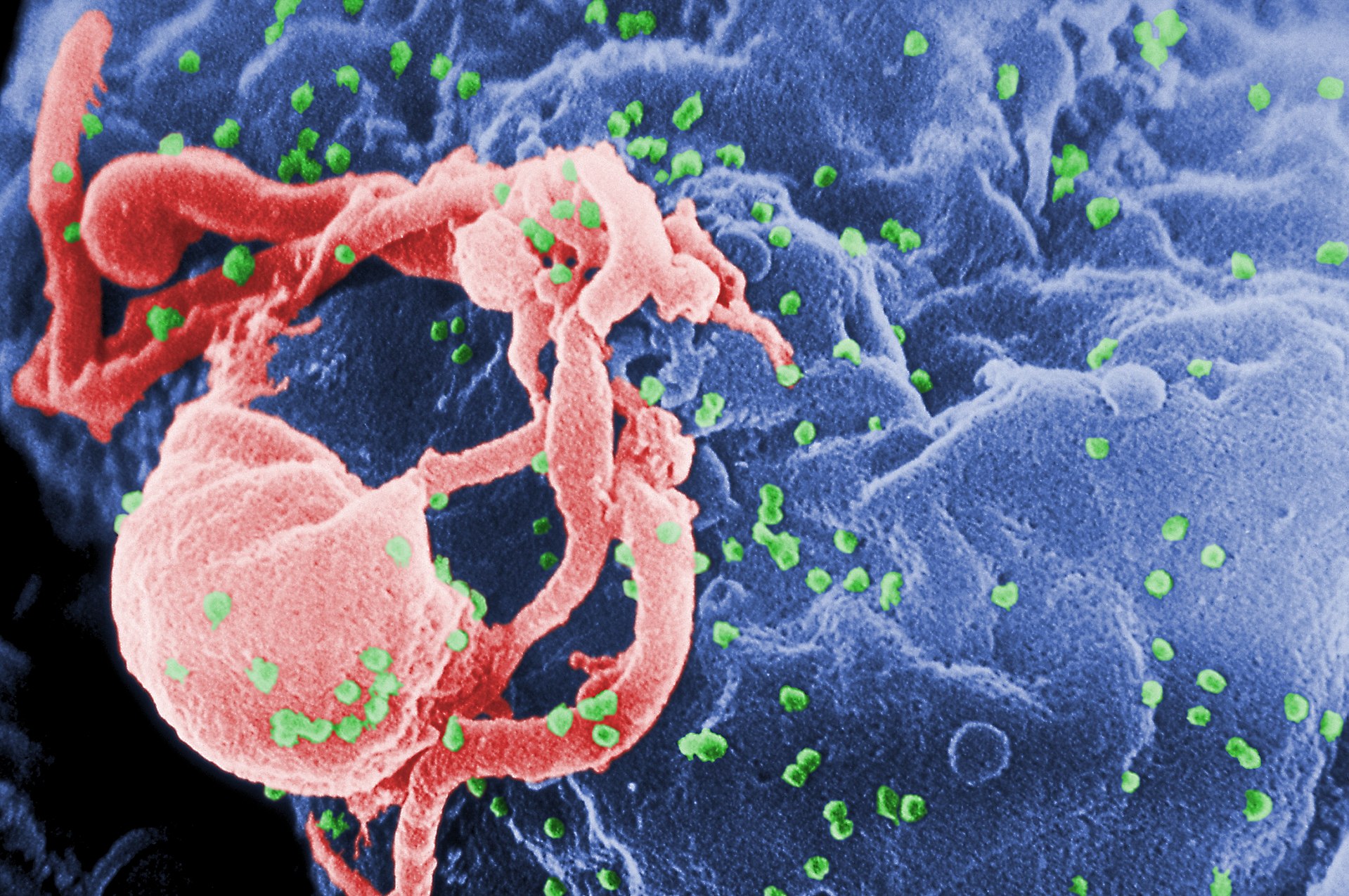
- Decreased life expectancy (74yr to 30yr in 2007)
- Almost no natural growth due to increased death rates
What are the social effects?
Families in poverty cannot afford the medical healthcare. Consequently the death rate is increasing and therefore:
- Psychological Effect (Children become orphans and are devastated due to parent loss.)
- Income drops due to loss of family. Children might not be able to get further education.
- People have a negative outlook on life when they get the virus.
- The population becomes paranoid of the virus.
- Increases the students per teacher and people per doctor ratios. This means less education and fewer chances of medical help.
- Families, particularly men, may in-migrate to meet the local demand for workers. The men may sleep with an HIV infected woman and bring the virus back into their hometown.
What are the economic effects?

- Orphaned children become dependent on non-working grandparents which leads to further poverty. Some may need to survive on their own by stealing.
- Decrease in industrial and agricultural productivity per capita leading to poverty and food shortages
- A lower life expectancy decreases the time and therefore amount of work a person is expected to do. The decreased pool of labor reverses the country’s economic growth.
- It has been projected that the economy of the country will be one third smaller in 2021 than it might have been without the epidemic (disease)
- The money that could be invested in the country’s infrastructure may be used instead to buy anti-retroviral drugs to cope with the virus’ stress on medical healthcare.
- It has been estimated that by 2010 total government funding in Health will have to increase by 20% on 2005 figure despite a reduction in the workforce
- Due to country’s social unreliability multinational companies prefer not to invest in the economy and tourists prefer not want to visit the country.
What is Botswana doing to combat the problem?

- In 2002 Botswana became the first African country to offer free condoms to its population
- Anti-retroviral drugs are provided by government clinics (tapping in to the wealth created from the Diamond industry in the country)
- More government money is going in to AIDS Education programmes
- The government’s spending on health will increase by 3% per year over the next 10 years.
- Free HIV tests are offered at local medical centers
- Botswana is working on high-tech food security initiatives, so for example they may use HYVs for crops to guarantee a food supply even though the number of farm laborers is decreasing.
View count: 10885